Vikram V Kadu, K A Saindane, Ninad Goghate, Neha N Godghate
Volume 1 | Issue 1 | April – Jun 2016 | Page 43-45
Author: Vikram V Kadu [1], K A Saindane [1], Ninad Goghate [1], Neha N Godghate [1]
[1] ACPM Medical College, Dhule – 424001, Maharashtra, India
Address of Correspondence
Dr. Vikram V. Kadu
ACPM Medical College, Dhule – 424001, Maharashtra India
Email : vikram1065@gmail.com
Abstract
Introduction:Arthroscopic reduction and internal fixation (ARIF) of tibial intercondylar eminence fractures is the emerging state-of-the-art. Tibial eminence fractures underwent arthroscopic evaluation when closed reduction after aspiration failed to yield an anatomic reduction. Arthroscopic reduction and fixation of avulsion fractures of the tibial eminence restores the length of the ACL, provides stable fixation promoting early motion.
Materials and Methods: This is a retrospective study conducted between 2010 and 2012. All 40 patients suffering ACL injury with tibial eminence fracture were stabilized in the emergency room followed by above knee slab. Once the patient was stabilized surgery (Arthroscopic reduction and internal fixation) was performed. The technique involved arthroscopic placement of a 3.5-mm cannulated compression screw into the tibial eminence. Patients were placed in a standard postoperative ACL protocol. Assessment was done using knee society score.
Result: All fractures demonstrated radiographic healing by 8 weeks, and none of the patients had subjective complaints of pain and instability. At 2 yrs follow-up all the patients had functional range of motion (00-1600) and returned successfully to their previous work. In our series we didn’t come across any complication.
Conclusion: Arthroscopic reduction and screw fixation with a cannulated screw is a simple, effective, and safe technique providing stable fracture fixation to allow immediate mobilization with minimal loss of extension.
Key words : ACL avulsion fracture, Arthroscopic, cannulated screw
Introduction
The intercondylar eminence serves as the point of attachment for portions of the menisci and the anterior and posterior cruciate ligaments(1). In addition to disrupting ACL continuity, intercondylar eminence avulsion fractures, depending on size, may affect weight-bearing aspects of the articular surface of the tibia.
Fracture of the tibial intercondylar eminence is a consequence of ACL avulsion at its insertion(2). Mechanism being same as of ACL rupture it is pulled from the tibia with a piece of the bony plateau. These injuries are commonly related to high energy trauma usually road traffic accidents and have high incidence of associated injuries.
Fractures of the tibial intercondylar eminence were classified into 3 types3: type I, minimal or nondisplaced; type II, partially displaced or hinged fracture; and type III, completely displaced. Surgical treatment is currently recommended for type II and III displaced fractures. Open methods were conventionally used to fix these avulsions however now arthroscopic treatment is the standard of care. Most of the existing literature is from the western world and publications from India are very few. We present our series of arthroscopic fixation done for ACL avulsion fracture performed at a district level rural center in India
Materials and Methods:
This is a retrospective study conducted on 40 patients suffering ACL injury with tibial eminence fracture between 2010 and 2012. Patients were stabilized in the emergency room followed by above knee slab. Of the 40 patients 27 were male and 13 female. 26 were right sided and 14 left sided. 28 suffered RTA and 12 had fall. Mean age of the patient was 35 yrs (range 23 – 47 yrs). After stabilizing the patient, surgery (Arthroscopic reduction and internal fixation with 3.5 mm screw) was performed. The technique involved arthroscopic placement of a 3.5-mm cannulated compression screw into the tibial eminence. Patients were placed in a standard postoperative ACL protocol. All patients were clinically and radiographically reviewed for 2 years and assessed with knee society score.
Surgical Technique:
In supine position with the knee flexed 70° to 90°. Pneumatic tourniquet was used. Standard knee arthroscopy was performed with anterolateral and anteromedial portals. In all patients, an additional antero-superior parapatellar portal was used for wider and better view of the intercondylar tibial eminence.

Figure 1: showing the entry portals.
Through the standard anteromedial portals, using Normal saline under gravity the hemarthrosis was washed out using the shaver, the hematomas at the fracture site were debrided, and the joint was inspected for the presence of any other intra-articular lesions. Turning the optics anteriorly, the intermeniscal ligament was identified, and in cases with interposition, the ligament was shifted aside using a probe introduced through the standard anteromedial portal to make reduction possible. Sometimes the ligament needs to be partially cut. After the anatomic condition and integrity of the ACL were carefully confirmed, the probe was then used via the anteromedial portal to reduce the fracture in its bony bed.
Under arthroscopic vision, the midpoint of the inferior non-articular surface of the patella is selected and a guide wire of 1.2 mm was then passed perpendicular to this surface, in the direction of the center of the fracture site with the knee flexed to approximately 70° to 90°. The portal was then drilled using a 2.7 mm cannulated drill bit and fragment was fixed with 3.5 mm cannulated screw.
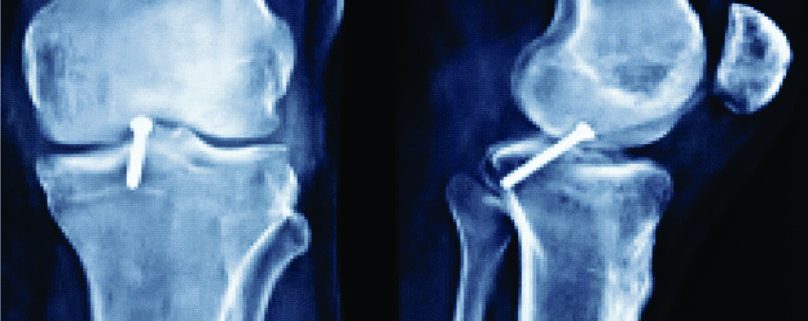
Case: 30 yrs old male labourer by occupation suffered an RTA and presented with complaints of pain and swelling over left knee joint and restriction of movements. Clinically the patient had instability at the knee joint. X-rays both AP and Lateral view were taken (Fig 2A) which showed fracture tibial eminence. The patient was given above knee slab and was admitted. Surgery (Arthroscopic reduction and internal fixation with 3.5 mm screw) was performed. Post- operatively the patient was given long leg knee brace. Physiotherapy in the form of Quadriceps exercises was started immediately and knee bending (upto 30 degrees) and partial toe touch bearing walking with walker with long leg knee race on post-op day 2 once the drain was removed. Patient was followed up after 1 month (Fig 2B). X ray showed uniting fracture. Knee bending was increased from 30-60 degrees and 50 % weight bearing allowed. At 2 months (Fig 2C) X ray showed radiological union and patient was advised full weight bearing walking with walker and brace, knee ROM exercises were started and complete flexion and extension was allowed. At 12 weeks (Fig 2D). X rays at 10 months follow-up (Fig 2E). At 2 yrs and 7 months follow up (Fig 2F). The patient has full range of motion (0-160o) (Fig 2G &H) and returned to his previous work.

Figure 2A: pre-op AP and LAT view

Figure 2B: Radiograph at 1 month follow-up

Figure 2C: Radiograph at 2 months follow-up

Figure 2D: Radiograph at 3 months follow-up

Figure 2E: Radiograph at 10 months follow-up

Figure 2F: Radiograph at 2yrs and 7 months follow-up

Figure 2G: Radiograph at 10 months follow-up

Figure 2H: Radiograph at 10 months follow-up
Observations and Results:
All the 40 patients were assessed at the end of 2 yrs and we found out that, all patients had functional range of movement of the knee joint and they returned to their previous work. There was no evidence of any infection or complication in our study. There was no failure of fixation and no other complications in our series
Discussion:
Tibial spine fractures usually result from a twisting movement of the knee. Abnormal valgus/varus or hyperflexion /hyperextension forces can cause avulsion of the tibial eminence. Such injuries are common after road traffic accidents or sporting activities.
Arthroscopic reduction internal fixation of intercondylar eminence avulsion is recommended for all displaced type III fractures and should be considered in all cases of displaced type II fractures. Various studies by different authors have been reported for these kind of fractures(2,4-10). Tibia eminence fracture results in anterior knee instability and occasionally anterior impingement during knee extension when the avulsion fragment is displaced(11). The goal of treatment for displaced tibial intercondylar eminence fracture is anatomic reduction. Disadvantages of screw fixation include risks of comminution of the fracture fragment, impingement due to prominent screw head, and the need for hardware removal. Because of these risks, some surgeons preferred arthroscopic reduction and internal fixation using non-absorbable sutures passed through drill holes. Suture techniques may obviate the need for a second surgery for implant removal and impingement; but arthrofibrosis and limitation of joint motion due to postoperative immobilization have been reported(2.) It has been found that antegrade screw fixation is more effective in obtaining initial rigid fixation than pull-out suture fixation for ACL avulsion fractures(12).
Tibial eminence fractures have excellent prognosis. Previously, prolonged immobilization may lead to arthrofibrosis and a permanent loss of full extension. Therefore, earlier rehabilitation is crucial as it encourages a faster recovery and prevents the development of secondary complications. Rehabilitation is similar to ACL tear protocols activities include static cycling, leg presses, elastic theraband or tubing exercises.
The technique described in this report not only helps achieve good interfragmentary compression, but also prevents undue prominence of the screw head owing to its proper direction. The bicortical purchase of the screw adds to the stability of fracture fixation, allowing early joint movement and weight bearing. The parapatellar portal secures good visualization of the operative field, enabling the screw to fix the fracture fragment perpendicularly. Although rare but chances of fracture in cases of poor bone quality is to be considered.
Conclusion
Arthroscopic reduction and internal fixation with cannulated screws for type 3B fractures having ACL injury is a novel method with good results and without any complications.
References
1. Wiss DA, Watson JT. Fractures of the tibial plateau. In:Rockwood CA, Green DP, Bucholz RW, Heckman JD, eds. Rockwood and Green’s fractures in adults.Philadelphia: Lippincott-Raven, 1996;1920-1953.
2. Berg EE. Comminuted tibial eminence anterior cruciate ligament avulsion fractures: Failure of arthroscopic treatment. Arthroscopy1993;9:446-450.
3. Meyers MH, McKeever FM. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am. 1970; 52(8):1677-1684.
4. McLennan JG. The role of arthroscopic surgery in the treatment of fractures of the intercondylar eminence of the tibia. J Bone Joint Surg Br1982;64:477-480.
5. Falstie-Jensen S, Sondergard Petersen PE. Incarceration of the meniscus in fractures of the intercondylar eminence of the tibia in children. Injury1984;15:236-238.
6. Matthews DE, Geissler WB. Arthroscopic suture fixation of displaced tibial eminence fractures.Arthroscopy1994;10:418-423.
7. Osti L, Merlo F, Bocchi L. Our experience in the arthroscopic treatment of fracture-avulsion of the tibial spine. Chir Organi Mov1997;82:295-299.
8. Kocher MS, Micheli LJ, Gerbino P, Hresko MT. Tibial eminence fractures in children: Prevalence of meniscal entrapment.Am J Sports Med2003;31:404-407.
9. Chandler JT, Miller TM: Tibial eminence fracture with meniscal entrapment.Arthroscopy1995;11:499-502.
10. Berg EE. Comminuted tibial eminence anterior cruciate ligament avulsion fractures: Failure of arthroscopic treatment. Arthroscopy1993;9:446-450.
11. Senekovic V, Veselko M. Anterograde arthroscopic fixation of avulsion fractures of the tibial eminence with a cannulated screw: Five-year results.Arthroscopy2003;19:54-61.
12. Kendall NS, Hsu SY, Chan KM. Fracture of the tibial spine in adults and children. A review of 31 cases. J Bone Joint Surg Br. 1992; 74(6):848-852.
13. Berg EE. Comminuted tibial eminence anterior cruciate ligament avulsion fractures: failure of arthroscopic treatment.Arthroscopy. 1993; 9(4):446-450.
14. Tsukada H, Ishibashi Y, Tsuda E, Hiraga Y, Toh S. A biomechanical comparison of repair techniques for anterior cruciate ligament tibial avulsion fracture under cyclic loading. Arthroscopy. 2005; 21(10):1197-1201.
| How to Cite this article: Kadu V V, Saindane K A, Goghate N, Godghate N N. Arthroscopic reduction and Internal fixation (ARIF) using Parapatellar Approach – A modality for treating fracture Tibial eminence with ACL injury . Asian Journal of Arthroscopy Apr- June 2016;1(1):43-45 . |
 Dr. Vikram V. Kadu |
 Dr. K. A. Saindane |
 Dr. Ninad Godghate |
 Dr. Neha N Godghate |
|